Key Takeaways
- DRC's 17th Ebola outbreak in 50 years. DRC declared its 17th Ebola outbreak on 15 May 2026, a Bundibugyo virus outbreak in Ituri Province. By 27 June it had grown to 1,294 confirmed cases (1,274 in DRC, 20 in Uganda) and about 362 confirmed deaths, making it the third-largest Ebola outbreak on record.
- WHO declared a global health emergency on 16 May. The Director-General's PHEIC declaration is the highest-level alert under International Health Regulations — only the 8th time it's been invoked since 2005.
- Two imported cases in Uganda. Uganda has confirmed 20 cases, including 2 deaths. The virus has also reached Europe through imported cases: an American doctor was airlifted to Berlin's Charité in May, and France confirmed an imported case on 24 June.
- No licensed vaccine for the Bundibugyo strain. Existing Ebola vaccines (Ervebo, Mvabea-Zabdeno) target the Zaire strain. Bundibugyo virus has caused only two prior outbreaks (2007 Uganda, 2012 DRC) — limited treatment options.
- 35,000+ cases globally since 1976. Roughly 80% from the 2014–2016 West Africa outbreak (Sierra Leone, Liberia, Guinea). DRC has now had 17 separate outbreaks — more than any other country.
On 16 May 2026, the World Health Organization declared the new Ebola outbreak in the Democratic Republic of the Congo a Public Health Emergency of International Concern (PHEIC) — the highest-level alert under the International Health Regulations and only the eighth such declaration since the framework’s modern adoption in 2005. The trigger: an outbreak of Bundibugyo virus disease in eastern DRC’s Ituri Province, with cross-border spread to Uganda and the first known intercontinental medical evacuation already underway.
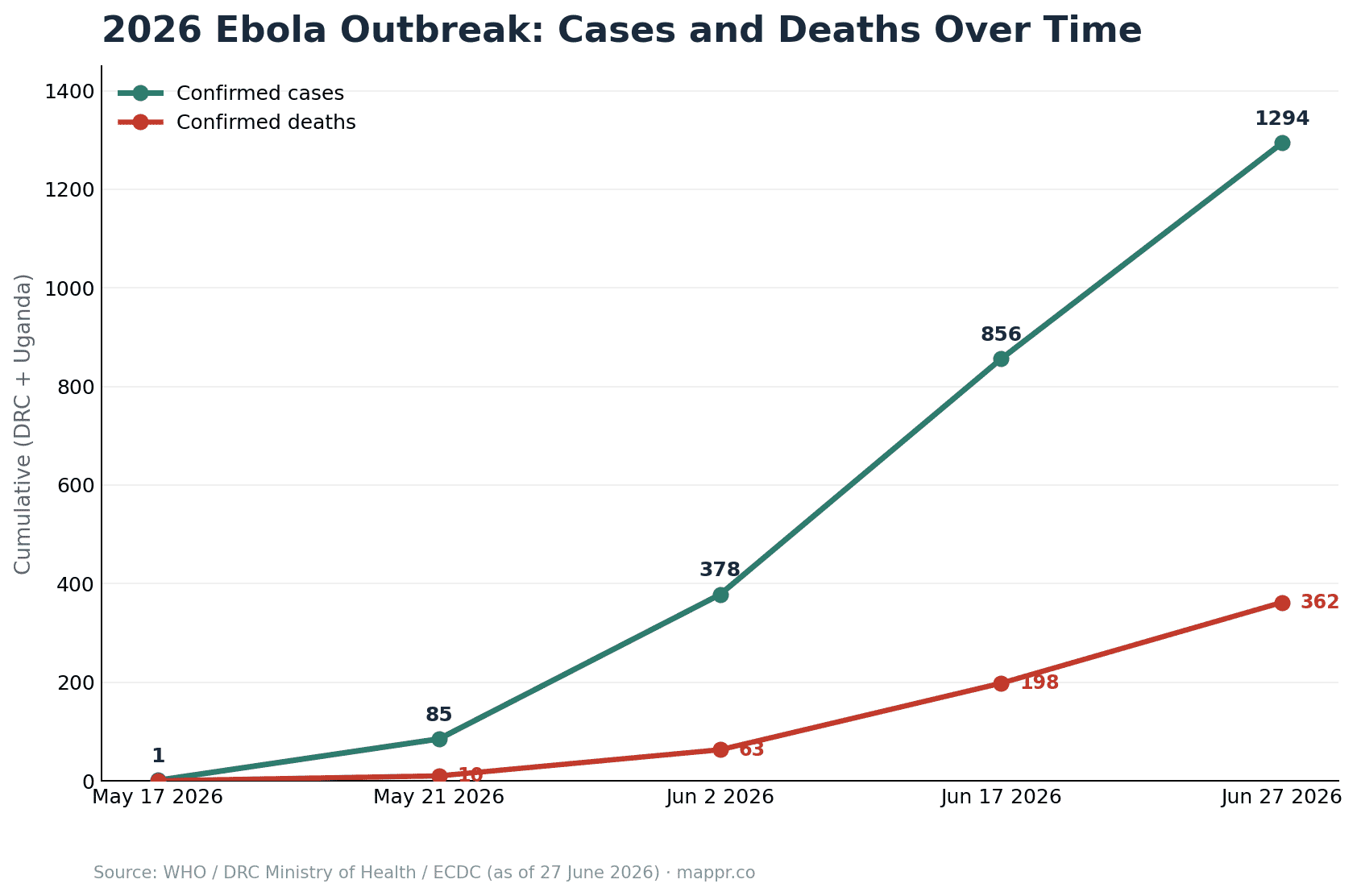
Latest figures (27 June 2026): the outbreak is still growing rapidly. The DRC Ministry of Health, WHO and ECDC report 1,294 confirmed cases and 362 confirmed deaths across DRC and Uganda (1,274 cases and 360 deaths in the DRC, plus 20 cases and 2 deaths in Uganda), a case-fatality rate of about 28%. Within the DRC, Ituri Province remains the epicentre with roughly 1,165 cases, followed by North Kivu (98) and South Kivu (3). That is up from 856 confirmed cases on 17 June and 378 on 2 June, making this the third-largest Ebola outbreak ever recorded. The virus has reached Europe twice through imported cases: an American missionary doctor, Peter Stafford, was airlifted from Nyankunde Hospital near Bunia to Berlin’s Charité hospital in May, and France confirmed an imported case on 24 June.
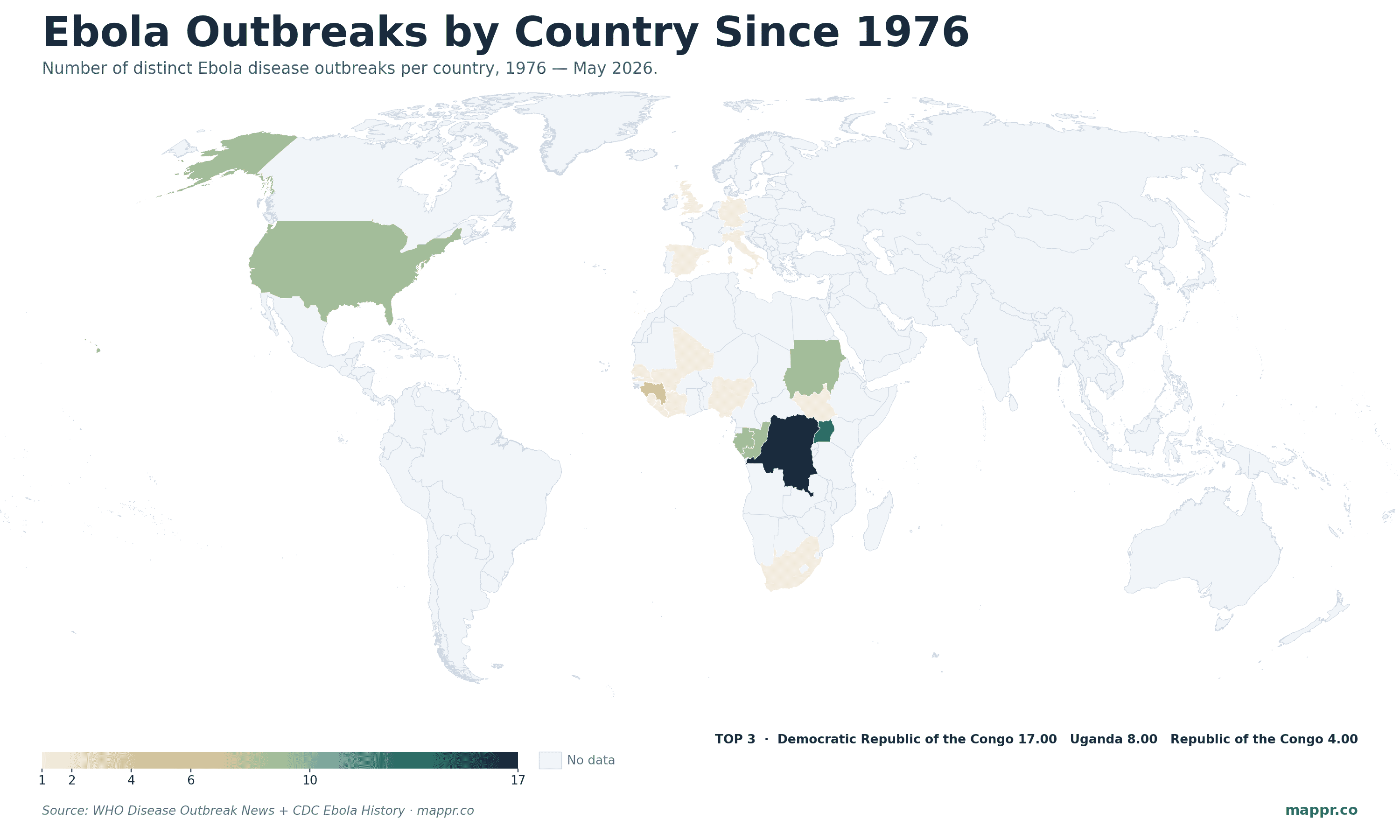
This is the 17th Ebola outbreak in the DRC since the virus was identified in the country in 1976 — the highest count of any nation. The map below shows the geography of all known Ebola outbreaks since then, with the DRC at the centre.
The Current Outbreak: A Timeline
- 24 April 2026 — A health worker in Bunia, Ituri Province, develops fever, vomiting, intense malaise, and signs of haemorrhagic illness. He dies at a medical centre in Bunia. Index case, retrospectively.
- 5 May 2026 — WHO receives an alert about an unknown high-mortality illness in Mongbwalu Health Zone, Ituri. Four healthcare workers have died within four days.
- 13 May 2026 — Rapid response teams complete in-depth investigations in Mongbwalu and Rwampara health zones. Initial Ebola Xpert testing on 20 Rwampara samples is negative; samples sent to Kinshasa for full PCR.
- 15 May 2026 — DRC’s national reference laboratory (Institut National de la Recherche Biomédicale) confirms Orthoebolavirus bundibugyoense by PCR and genomic sequencing. DRC Ministry of Public Health officially declares the country’s 17th Ebola outbreak.
- 15 May 2026 — Uganda’s Ministry of Health confirms a Bundibugyo virus case in an elderly man admitted to a Kampala private hospital on 11 May; he died on 14 May. His body was returned to DRC the same day.
- 16 May 2026 — A second imported case is confirmed in Kampala. The WHO Director-General, following IHR consultation, declares Ebola in DRC and Uganda a PHEIC.
- 18 May 2026 — The US CDC, DHS, and federal partners implement enhanced traveller screening and entry restrictions.
- 29 May 2026 — Case totals climb to 125 confirmed and 906 suspected cases, with 223 suspected deaths; the Africa CDC reports more than 1,000 suspected cases in DRC alone, and WHO’s Director-General travels to the outbreak epicentre.
- 2 June 2026 — Confirmed cases reach 378 (363 in DRC, 15 in Uganda) with 63 confirmed deaths as transmission accelerates across Ituri.
- 17 June 2026 — The outbreak reaches 856 confirmed cases and 198 confirmed deaths; Ituri Province accounts for 767 cases, with spread into North Kivu and South Kivu.
- 24 June 2026: France confirms an imported Ebola case, the outbreak’s second to reach Europe after the May evacuation to Germany.
- 27 June 2026: Cumulative totals pass 1,294 confirmed cases and 362 confirmed deaths across DRC and Uganda, making this the third-largest Ebola outbreak on record; Ituri Province remains the epicentre (about 1,165 cases).
Where the Outbreak Started — and Why It Spread
The current epicentre is Mongbwalu Health Zone in Ituri Province, a high-traffic mining area in eastern DRC. WHO’s epidemiologists believe most early cases originated there, then migrated to Rwampara and Bunia health zones in search of medical care — bringing the virus into population centres with imperfect infection control.
Three features make Ituri a particularly high-risk launch point for regional spread:
- Mining and commercial traffic — Mongbwalu is a regional gold-mining hub with extensive informal labour movement.
- Cross-border proximity — Ituri shares borders with Uganda and South Sudan; Bunia HZ is less than 500 km from the Ugandan border. Two imported Uganda cases in less than a week confirm this concern.
- Insecurity — Active armed groups in parts of Ituri have limited the rapid-response team’s ability to identify and follow up contacts. As of 15 May, 65 contacts had been listed, 15 high-risk, but several had become symptomatic and died before they could be isolated.
The Outbreak Spreads Beyond DRC
Within ten days of the WHO’s PHEIC declaration, the outbreak has produced its first intercontinental cases — none yet from local transmission, but several through cross-border movement of patients and aid workers.
- 🇺🇬 Uganda — 19 confirmed cases, 2 deaths. Up from 2 in the immediate aftermath of the PHEIC, mostly in Kampala plus one in Wakiso district. The initial Kampala case died on 14 May; subsequent cases include healthcare workers and travellers returning from Ituri Province. No sustained local Ugandan transmission has been documented yet, but the chain length is growing.
- 🇩🇪 Germany — 1 evacuated American case at Berlin’s Charité. Peter Stafford, a US missionary doctor who has worked at Nyankunde Hospital in eastern DRC since 2019, contracted Bundibugyo virus while treating Ebola patients. He was airlifted to Berlin-Brandenburg airport on 19 May 2026 and transferred under police convoy to Charité’s specialised isolation ward (the same unit that treated patients during the 2014–2016 West Africa outbreak). Six high-risk contacts will be monitored in Germany and the Czech Republic. This is the first known Ebola medical evacuation to Europe in the current outbreak.
- 🇺🇸 United States — enhanced screening, no cases. CDC, DHS, and partner agencies implemented Title-42-style entry restrictions on 18 May for travellers from DRC and Uganda. Departure-airport screening, on-arrival temperature checks, and 21-day post-arrival monitoring are now standard for entries from the affected region. No US-soil cases have been reported.
The American patient’s evacuation puts a fact often missed in headlines into sharp relief: Ebola containment depends as much on the global health workforce as on local capacity. Stafford was one of the international clinicians sustaining frontline care at Nyankunde Hospital — the same kind of role that, during the 2014–2016 West Africa outbreak, saw infections among foreign medical workers in MSF, the US Public Health Service, and Spanish and Italian missionary hospitals. The Charité has handled four previous Ebola patient evacuations across the 2014–2016 and 2018–2020 outbreaks; the unit’s protocols are well-established, and the patient prognosis (the Bundibugyo strain’s case-fatality is roughly 30–40%, lower than Zaire ebolavirus) is comparatively favourable with intensive supportive care.
WHO’s Director-General used the word “serious concern” on 19 May to describe the trajectory. WHO’s DRC representative told reporters there is “significant uncertainty” about how far the virus has actually spread — contact tracing in Ituri is being run under conditions of active insecurity and intermittent road closures, and several listed contacts have died before they could be isolated, suggesting transmission chains are longer than the confirmed case count implies.
What Bundibugyo Virus Is
Ebola is not a single virus. The genus Orthoebolavirus contains six recognised species, of which four are known to cause disease in humans. The most-studied — and the target of all licensed vaccines — is Zaire ebolavirus (EBOV), which causes the highest case-fatality rates (up to 90% untreated) and has driven the largest outbreaks, including the 2014–2016 West Africa epidemic and the 2018–2020 DRC outbreak.
The current outbreak is Bundibugyo virus (BDBV), the rarest of the four human-pathogenic species. Discovered in 2007 during an outbreak in western Uganda’s Bundibugyo District, it has caused only two prior outbreaks — Bundibugyo District 2007 (149 cases) and Isiro Health Zone, DRC, 2012 (52 cases). Case-fatality is around 30–40%, lower than Zaire ebolavirus but still extremely high.
Critically, the two licensed Ebola vaccines — Ervebo (rVSV-ZEBOV) and the Mvabea/Zabdeno two-dose regimen — both target Zaire ebolavirus. Cross-protection against Bundibugyo virus has not been clinically established. The two monoclonal antibody treatments (Inmazeb and Ebanga) also target Zaire-specific epitopes. Standard Ebola medical countermeasures may not work against this strain; the response is relying on classic outbreak containment (case isolation, contact tracing, safe burials) rather than vaccination.
Ebola Cases Worldwide Since 1976
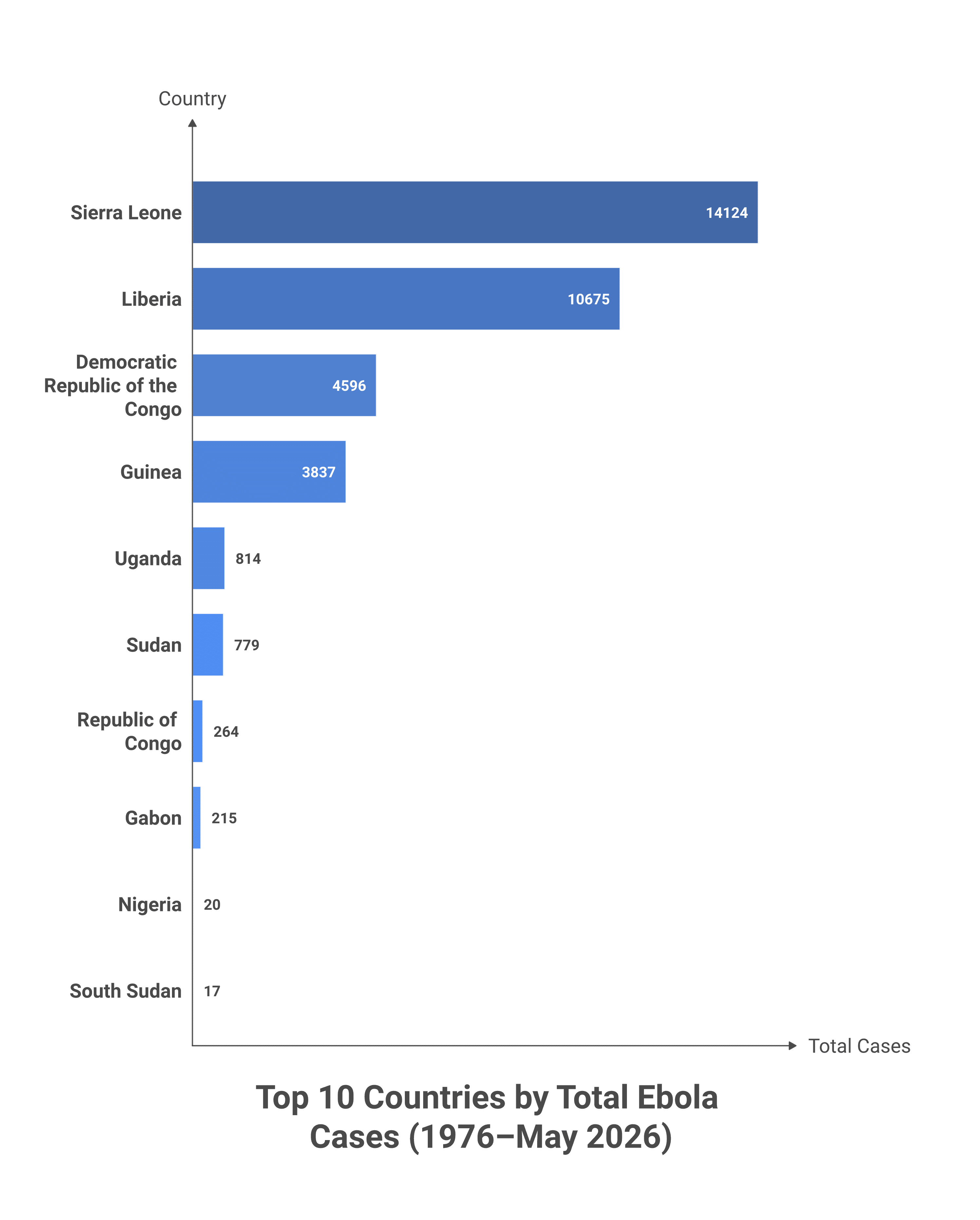
Since Ebola was first identified in 1976 in what is now the DRC, roughly 35,000 cases have been recorded across 19 countries — but the distribution is extremely skewed. The 2014–2016 West Africa outbreak alone accounts for about 80% of the cumulative case total, with three countries (Sierra Leone, Liberia, Guinea) carrying most of it.
Outbreak history · 1976–2026
Ebola outbreaks by country
Reported outbreaks, cumulative cases, and deaths across every affected country since the virus was first identified. 2026 figures include the ongoing DRC and Uganda outbreaks.
| Country | Outbreaks | Cases | Deaths | Years |
|---|---|---|---|---|
| Democratic Republic of the Congo | 17 | 4,596 | 2,738 | 1976–2026 |
| Uganda | 8 | 814 | 322 | 2000–2026 |
| Sierra Leone | 1 | 14,124 | 3,956 | 2014–2016 |
| Liberia | 1 | 10,675 | 4,809 | 2014–2016 |
| Guinea | 2 | 3,837 | 2,545 | 2014–2021 |
| Sudan | 4 | 779 | 432 | 1976–2004 |
| Republic of the Congo | 4 | 264 | 211 | 2001–2005 |
| Gabon | 4 | 215 | 165 | 1994–2002 |
| Nigeria | 1 | 20 | 8 | 2014 |
| South Sudan | 1 | 17 | 7 | 2004 |
| Mali | 1 | 8 | 6 | 2014 |
| South Africa | 1 | 2 | 1 | 1996 (import from Gabon) |
| Ivory Coast | 1 | 1 | 0 | 1994 (Taï Forest virus) |
| Senegal | 1 | 1 | 0 | 2014 (import) |
| United States | 4 | 11 | 2 | 1989–2015 (imports + Reston strain in macaques) |
| United Kingdom · Spain · Italy · Germany | 1each | 1each | 0 | 2014–2015 (healthcare-worker imports) |