Key Takeaways
- 240 million people live with chronic Hepatitis B. The WHO's Global Hepatitis Report 2026 (released April 2026) estimates 240 million chronic HBV cases globally — fewer than 5% of whom are receiving treatment. Hepatitis B and C together account for over 95% of viral hepatitis deaths worldwide.
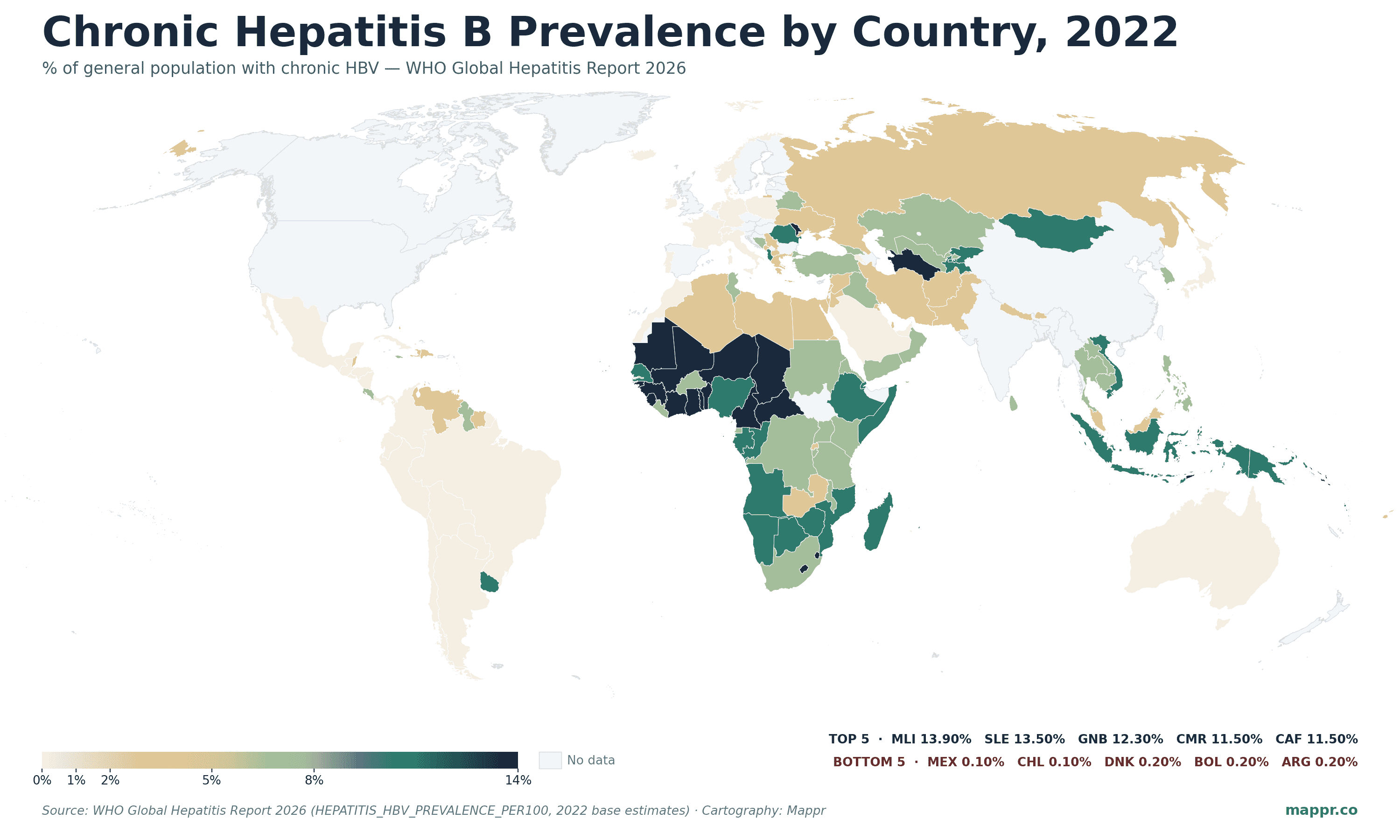
- West Africa has the world's highest prevalence. Mali (13.9%), Sierra Leone (13.5%), Guinea-Bissau (12.3%), Central African Republic (11.5%), Cameroon (11.5%), and Benin (11.2%) all have more than one in nine adults living with chronic HBV. The Western Pacific is the second hotspot.
- Indonesia and Nigeria carry the largest absolute burden. Indonesia leads the world with 17.5 million people living with chronic HBV, followed by Nigeria (14.4M), Ethiopia (7.7M), Vietnam (6.5M), and the Philippines (5.7M). High prevalence + large populations make these the priority countries for treatment scale-up.
- Western Europe and the Americas sit below 1%. Most of Western Europe (Germany 0.3%, France 0.3%, Netherlands 0.3%, Norway 0.3%, Denmark 0.2%, Ireland 0.4%, Portugal 0.4%) and Latin America (Mexico 0.1%, Chile 0.1%, Argentina 0.2%, Bolivia 0.2%, Brazil 0.5%) report prevalence under 1% — the result of universal infant vaccination programs going back to the 1990s.
The World Health Organization’s Global Hepatitis Report 2026, released at the World Hepatitis Summit on April 28, 2026, is the first major dataset update on chronic Hepatitis B in years. The headline numbers are sobering: 240 million people live with chronic HBV worldwide, fewer than 5% are receiving treatment, and Hepatitis B and C together account for more than 95% of all deaths from viral hepatitis. Despite that scale, country-level prevalence is rarely mapped — most public discussion focuses on HIV, malaria, and tuberculosis, which have lower global infection counts.
This map uses the WHO’s chronic Hepatitis B prevalence indicator — the share of each country’s general population living with chronic HBV — with 2022 base-year estimates from the April 2026 report covering 167 countries. The geography is dramatic: a band of West African countries with prevalence above 10%, an Eastern and Southern African band above 5%, a cluster in the Western Pacific (Indonesia, Vietnam, Philippines, Solomon Islands), and almost everywhere else under 2%.
The Highest-Prevalence Countries: West Africa Above 10%
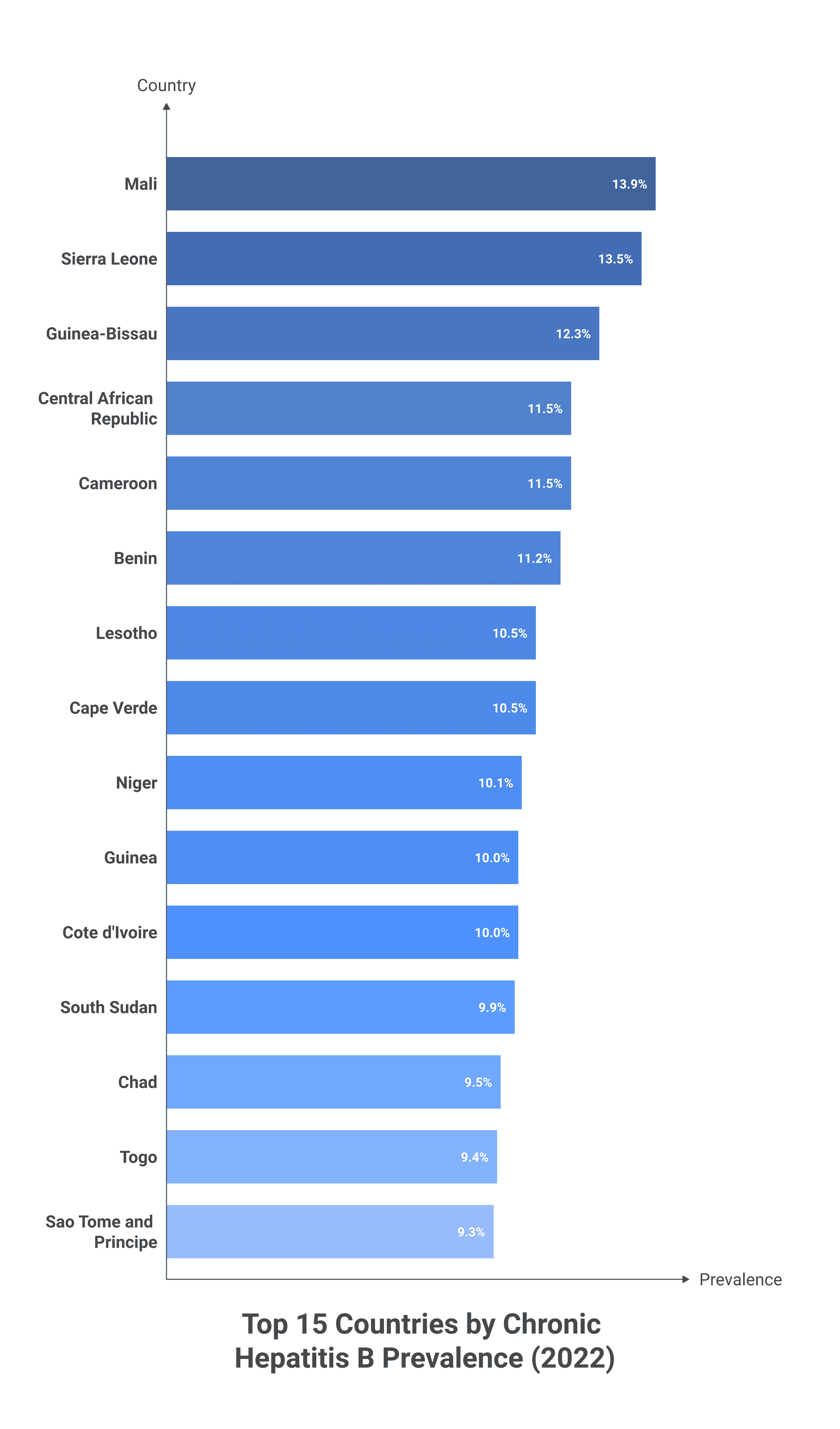
The top of the prevalence ranking is geographically concentrated. Of the 15 countries with chronic HBV prevalence above 9%, 13 are in West, Central, or Southern Africa.
| Country | HBV Prevalence (2022) | Region |
|---|---|---|
| 🇲🇱 Mali | 13.9% | West Africa |
| 🇸🇱 Sierra Leone | 13.5% | West Africa |
| 🇬🇼 Guinea-Bissau | 12.3% | West Africa |
| 🇨🇫 Central African Republic | 11.5% | Central Africa |
| 🇨🇲 Cameroon | 11.5% | Central Africa |
| 🇧🇯 Benin | 11.2% | West Africa |
| 🇱🇸 Lesotho | 10.5% | Southern Africa |
| 🇨🇻 Cape Verde | 10.5% | West Africa |
| 🇳🇪 Niger | 10.1% | West Africa |
| 🇬🇳 Guinea | 10.0% | West Africa |
| 🇨🇮 Côte d’Ivoire | 10.0% | West Africa |
| 🇸🇸 South Sudan | 9.9% | East Africa |
| 🇹🇩 Chad | 9.5% | Central Africa |
| 🇹🇬 Togo | 9.4% | West Africa |
| 🇸🇹 São Tomé and Príncipe | 9.3% | Central Africa |
The pattern is partly historical (HBV transmits horizontally between children in early life, and in much of West Africa universal infant vaccination only became standard in the 2000s) and partly structural (low birth-dose hepatitis B vaccine coverage means a substantial fraction of new infections happen via mother-to-child transmission at delivery — a gap the WHO 2030 elimination targets specifically address).
Where the Largest Numbers Live: Indonesia, Nigeria, Ethiopia
Prevalence rates tell one story; absolute numbers tell another. The countries with the largest numbers of people living with chronic HBV are a mix of high-prevalence small-population countries (where high % × small N = small total) and lower-prevalence large-population countries (where mid-single-digit % × big N = enormous total).
| Country | People living with chronic HBV (2022) | Prevalence |
|---|---|---|
| 🇮🇩 Indonesia | 17.5 million | 6.4% |
| 🇳🇬 Nigeria | 14.4 million | 6.6% |
| 🇪🇹 Ethiopia | 7.7 million | 6.2% |
| 🇻🇳 Vietnam | 6.5 million | 7.2% |
| 🇵🇭 Philippines | 5.7 million | 4.9% |
| 🇵🇰 Pakistan | 3.8 million | 1.6% |
| 🇬🇭 Ghana | 2.9 million | 9.0% |
| 🇨🇩 DR Congo | 2.8 million | 2.8% |
| 🇿🇦 South Africa | 2.7 million | 4.6% |
| 🇦🇴 Angola | 2.7 million | 7.6% |
| 🇳🇪 Niger | 2.6 million | 10.1% |
| 🇰🇪 Kenya | 2.4 million | 4.7% |
| 🇨🇮 Côte d’Ivoire | 2.2 million | 10.0% |
| 🇲🇿 Mozambique | 2.0 million | 5.9% |
| 🇸🇩 Sudan | 2.0 million | 4.4% |
Indonesia is the world’s largest single-country HBV cohort by a wide margin — 17.5 million people, more than 6% of the population. This drives the Western Pacific share of the global burden: WHO data attributes roughly 30% of the world’s chronic HBV cases to the WHO Western Pacific Region, with Indonesia alone accounting for the bulk.
Note that several major economies — China, India, the United States, the United Kingdom — do not appear in this table because they are not in the WHO GHO indicator dataset under the same code (these countries report HBV burden through other surveillance channels). External modelling estimates put China at ~75 million people living with chronic HBV (roughly 5% of population) and India at ~40 million (roughly 3%); both would change the ordering above considerably if folded in.
The Lowest-Prevalence Countries: Western Europe and Latin America
At the other end of the distribution, most of Western Europe and Latin America report prevalence under 1% — in many cases under 0.5%. The reason is consistent: universal infant Hepatitis B vaccination programs that started in the late 1980s through the 1990s in most high-income countries, with three-dose coverage now sustained above 95% in the populations these data cover.
- Latin America under 0.5%: Mexico (0.1%), Chile (0.1%), Argentina (0.2%), Bolivia (0.2%), Honduras (0.3%), Panama (0.3%), Peru (0.4%), Brazil (0.5%)
- Western Europe under 0.5%: Denmark (0.2%), Norway (0.3%), Netherlands (0.3%), France (0.3%), Germany (0.3%), Ireland (0.4%), Portugal (0.4%), Italy (0.5%)
- Australia & Japan: Australia 0.7%, Japan 0.8% — slightly higher reflecting earlier vaccine coverage gaps
- Saudi Arabia 0.8%: dramatic decline from the 1980s when Saudi prevalence exceeded 6%, driven by routine infant vaccination introduced in 1989
- Egypt 1.0%: low for the region, the result of an aggressive 2018–2024 universal Hepatitis B + C screen-and-treat program
The 2030 Elimination Target: Far Off Without a Treatment Surge
The WHO’s official goal is elimination of viral hepatitis as a public health threat by 2030 — defined as a 90% reduction in new cases and a 65% reduction in mortality from a 2015 baseline. The April 2026 report’s headline finding is that progress is well off track. Of the 240 million people living with chronic HBV globally, fewer than 5% are receiving any antiviral treatment — far below the 80% treatment-coverage target set for 2030. Birth-dose vaccine coverage in the African Region remains under 20%, against a 90% target. The global 2030 trajectory now points to elimination some time in the 2050s under current intervention levels.
The disconnect between the disease’s scale (more chronic cases globally than HIV and tuberculosis combined) and the policy response (a fraction of the funding HIV receives) is the report’s central editorial point. Increased birth-dose vaccine coverage in West Africa, Pakistan, and Indonesia, plus generic-tenofovir treatment scale-up, would do more to bend the global curve than any other single intervention according to the WHO modelling.
Data Caveats
Three caveats are important for anyone using this dataset for analysis or comparison.
2022 base year. The April 2026 WHO report uses 2022 estimates as the most recent comprehensive vintage. Country-level updates trickle in faster, but the comparative cross-country snapshot is built from 2022 data.
WHO data coverage gaps. The WHO’s chronic HBV prevalence series covers 167 countries — but several major HBV-burden countries (China, India, the United States, the United Kingdom) report their hepatitis surveillance through other channels and aren’t in this specific dataset. The map shows them as “no data” even though the underlying disease burden is well-characterised in country-specific studies.
Modelled estimates, not direct surveillance. Most country-level HBV prevalence figures come from serosurveys + statistical modelling rather than universal testing. Confidence intervals around the point estimates can be wide — particularly for countries without recent national surveys. The ordering of the top 15 is robust; the precise decimal rankings between adjacent countries are not.